You can run the cleanest Google Business Profile in your zip code. Rank number one for “fee-for-service dentist near me.” Spend $8,000 a month on marketing that actually works.
But if your front desk treats a $14,000 implant consult like an insurance verification call, none of it matters.
Knowing how to hire dental staff for an FFS practice isn’t just harder than hiring for a PPO office. It’s a different job entirely.
PPO practices run on volume, so a mediocre hire gets absorbed by the schedule.
Fee-for-service practices run on value, case acceptance, and patient relationships. Your team isn’t operating the practice. Your team is the practice.
That means:
- Your front desk has to defend fees without flinching when patients ask, “do you take my insurance?”
- Your treatment coordinator has to present $5,000 to $50,000 cases without apologizing for the number
- Your hygienist has to advocate for treatment, not just clean teeth and rebook in six months
- Your culture has to attract A-players, because the B-players cost you cases, not just productivity
Staffing is tied for the #1 challenge dental practices face heading into 2026, right alongside insurance issues, per the latest ADA Health Policy Institute data. For fee-for-service practices, the stakes are higher because every patient interaction is worth more.
This guide is the playbook I’ve used with FFS clients to fix hiring, training, and retention. Not generic dental hiring advice. The specific, contrarian moves that work for practices that don’t take insurance assignment, are transitioning out of PPO, or built their model on out-of-network from day one.
Let’s start with why this is a different game.
Why Is Hiring For A Fee-For-Service Practice Different Than Hiring For PPO?
Hiring for a fee-for-service practice is different because the job itself is different. PPO practices optimize for throughput. Fee-for-service practices optimize for value.
Same job titles, completely different work.
Here’s the breakdown.
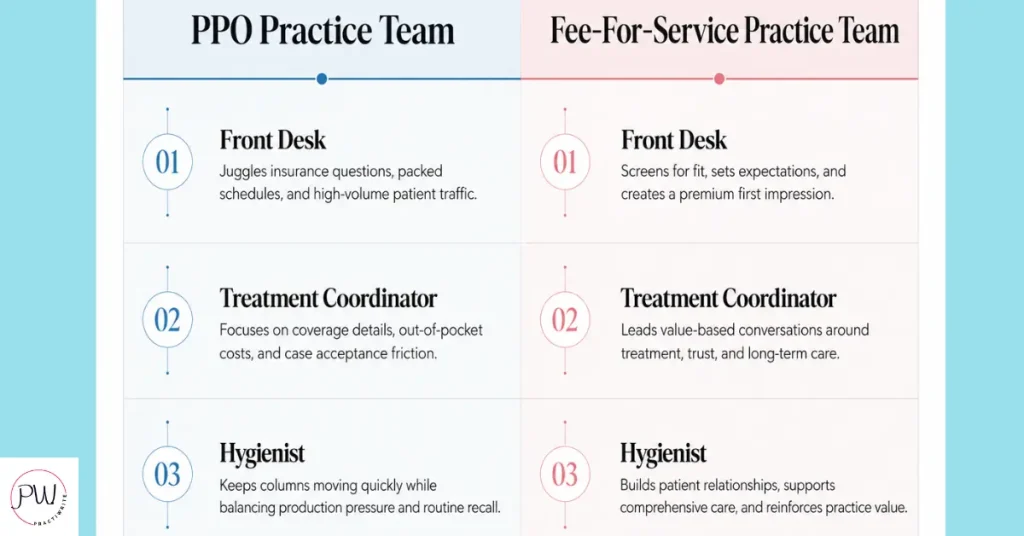
The Difference Between PPO vs FFS Practice Front Desk Hiring
The PPO front desk verifies insurance, processes claims, and runs the schedule like an assembly line. The FFS front desk explains why the practice doesn’t take assignment, defends the fee schedule, and converts price-shoppers into booked exams.
The PPO treatment coordinator estimates patient portions and walks patients through copays. The FFS treatment coordinator presents cases worth tens of thousands and helps patients say yes to paying out of pocket.
The PPO hygienist runs prophy after prophy on a 50-minute clock. The FFS hygienist has 60 to 90 minutes per patient, identifies same-day treatment opportunities, and builds the kind of relationship that drives referrals.
Same titles. Same licenses. Completely different skill stack.
Most Dental Front Desk Hiring Advice is Made for PPO Practices
The truth is, most dental hiring advice treats every practice like a PPO mill. That’s why your job postings sound like every other practice’s job postings, and that’s why you keep hiring people who can’t do the FFS job.
If your job posting says “fast-paced environment” and “high-volume practice,” you’re recruiting PPO staff for an FFS practice. They’ll quit within six months…..or you’ll wish they had.
The KPIs shift too. PPO practices track room turnover, calls answered, claims filed per hour. FFS practices track case acceptance rate, production per patient, and patient retention rate. The numbers that matter aren’t the same.
So why does almost every dental hiring guide treat fee-for-service and PPO practices like they’re hiring for the same job? Because writing one generic guide is easier than writing two specific ones.
That doesn’t help you. We’re going to do this the hard way.
What Should A Fee-For-Service Dental Job Description Say?
A fee-for-service dental job description should signal in the first two lines that this is not a PPO practice. Candidates self-select in or out based on whether they can sell value, hold fees, and thrive in a smaller, higher-margin environment.
I get it, you’ve got an opening to fill and you want to cast a wide net. But a wide net catches the wrong fish. Let me show you what works.
Lead with the practice type, explicitly. Not “patient-centered” or “modern practice,” because every office in America claims that. Use “fee-for-service” or “out-of-network” in the first sentence.
The candidates who can do the job will lean in. The ones who can’t will scroll past. That’s the point.
Specific Traits To List In Your Posting
- Comfort presenting fees in the $5,000 to $50,000 range without scripts
- Experience with longer appointment formats (60 to 90 minutes)
- Confidence handling “do you take my insurance” calls without losing the patient
- Clinical fluency that supports value-based treatment discussions
- A genuine interest in dentistry as a relationship business, not a transaction business
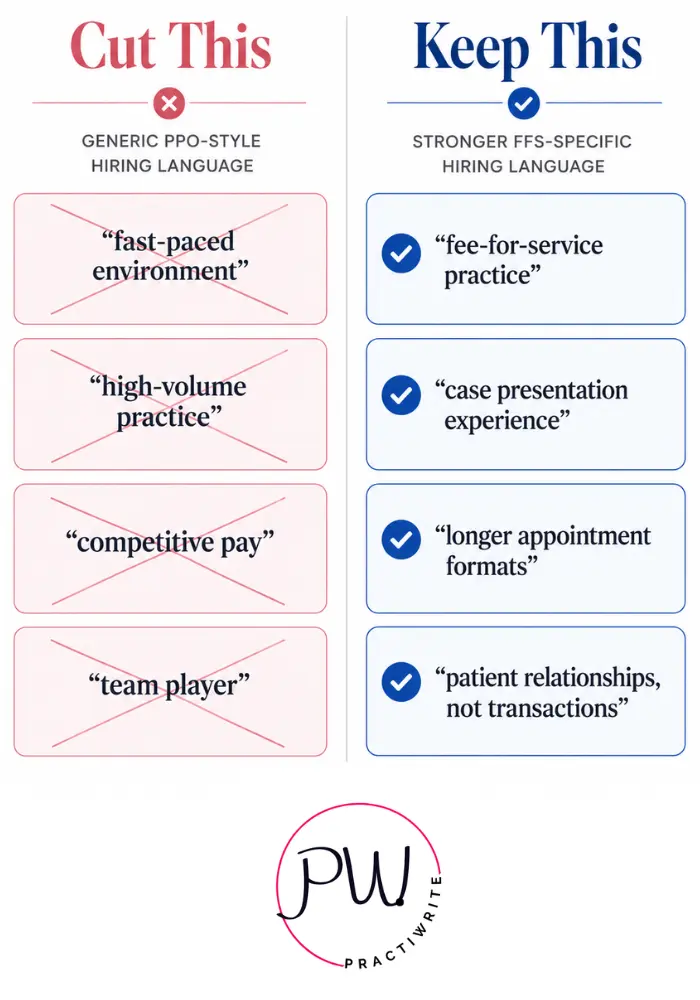
Phrases To Cut From Your Old Posting
- “Fast-paced environment” (PPO code)
- “High-volume practice” (PPO code)
- “Competitive pay” (every posting says this, means nothing)
- “Team player” (vague, filters for no one)
Where To Post For FFS Candidates
- DentalPost has FFS-specific filters most practices never use
- AADOM (American Association of Dental Office Management) for practice managers and treatment coordinators
- Your own GBP and website career page (Google indexes these, and FFS-curious candidates search for you specifically)
- Local dental hygiene programs, where new grads haven’t been broken by PPO mills yet
- LinkedIn for passive candidates who already work in FFS practices
The DentalPost 2025 Salary Report found that the mean hourly wage for dental practice managers rose 4.7% to $36.03 in 2024. For FFS practices, expect to pay above that average, because your margin allows it and your A-player candidates know their market value.
When was the last time you rewrote your job posting from scratch instead of editing the 2019 version?
How Do You Interview A Candidate For A Fee-For-Service Practice?
You interview a fee-for-service candidate by testing the skills the role actually requires. A resume can’t show you whether someone can hold a fee. A structured interview with live scenarios can.
Most practices interview like they’re hiring for the wrong job. They ask about software, certifications, and “tell me about yourself.” That tells you nothing about whether the candidate can do the FFS work.
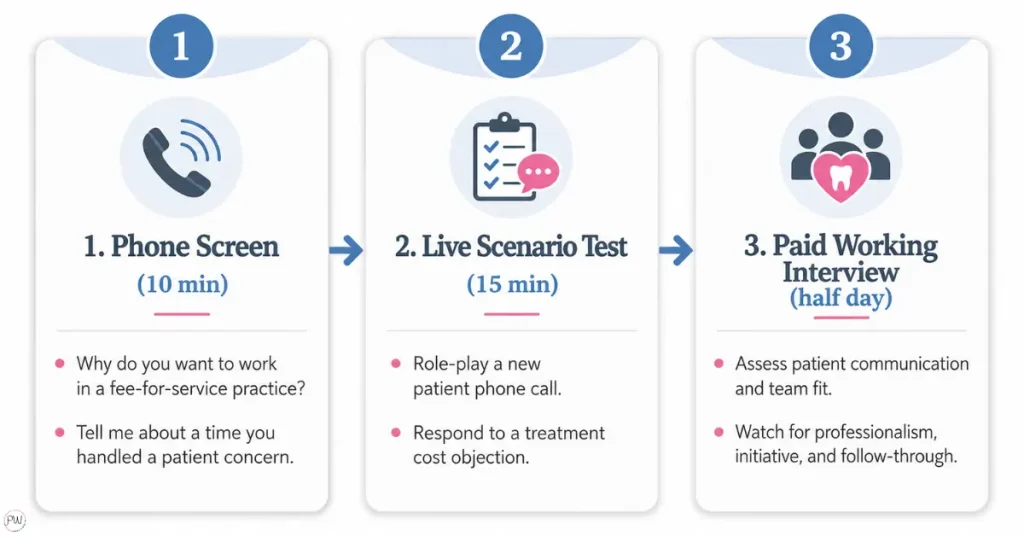
Here’s the three-step structure that actually filters.
Step 1: The 10-Minute Phone Screen
Two questions only.
- “Why are you interested in working at a fee-for-service practice specifically?” (Tests whether they understand the model)
- “Walk me through how you’d handle a call where the patient asks, ‘do you take my insurance?'” (Tests communication under pressure)
If they can’t answer either question confidently, the interview ends there. You just saved yourself two hours.
Step 2: The Live Scenario Test
Bring strong candidates in and run a 15-minute role-play. Use real situations:
- A patient pushing back on a $4,200 crown
- A phone shopper comparing your fee to the practice down the street
- A treatment coordinator handoff from a hygienist who spotted decay during cleaning
You’re not testing for perfect answers. You’re testing for poise, value-based language, and the ability to hold a fee without apologizing.
Step 3: The Paid Working Interview
Half a day in your practice, with a real value-presentation moment. Pay them for their time. Watch how they interact with patients, how they handle the team, and what they do in the moments that aren’t scripted.
Industry data shows case acceptance rates for general dentistry average 40-50% for existing patients and 25-35% for new patients, while top-performing practices hit 70-90%, per Practice by Numbers benchmarks.
The difference between those numbers isn’t the dentist. It’s the treatment coordinator and the front desk. If you’re hiring those roles based on a resume and a polite conversation, you’re hiring on hope.
Red Flags Specific To FFS Hiring
- “I just need a job” energy (they’ll leave the moment a PPO office offers $2 more an hour)
- Discomfort discussing fees out loud during the interview
- Defaulting to “I’d ask the doctor” instead of owning the conversation
- Bad-mouthing previous patients or practices (they’ll do the same to yours)
- Hesitancy when you ask about presenting cases over $10,000
Would you hire a sales rep without ever asking them to sell you something? Then why would you hire a treatment coordinator that way?
What Does Training Look Like For A Fee-For-Service Dental Team?
Training for a fee-for-service dental team focuses on value presentation, fee defense, and patient communication, not just software and policy. Your team needs to know how to explain why your practice is worth paying for out-of-pocket, in language that doesn’t sound salesy, defensive, or apologetic.
Most dental practices treat training like a one-week checklist. Shadow Sarah for three days, watch a HIPAA video, read the office manual, you’re good.
That works at a PPO mill where the job is mostly process execution. It fails at an FFS practice where the job is mostly conversation.
Here’s what actually works.
Build A 30/60/90 Day Onboarding Plan
Days 1-30: Practice systems, software, clinical fluency for the role. This is the boring stuff. Get it out of the way fast so you can spend the next 60 days on the work that matters.
Days 31-60: Value presentation training. Scripts for the “do you take my insurance” call. Scripts for the case presentation handoff. Scripts for the fee discussion. Then role-play with the team until the scripts sound natural, not robotic.
Days 61-90: Live patient interactions with feedback. Real cases, real conversations, real coaching. You or your office manager debriefs every meaningful interaction in the first month of patient contact.
Topics PPO Offices Skip That FFS Offices Must Train On
- How to explain why your fees are higher than the corporate chain down the road
- How to handle “I’ll have to check with my spouse” without losing the case
- How to present financing options without making the patient feel broke
- How to follow up on unscheduled treatment without sounding like a debt collector
- How to handle competitive offers from PPO practices that just hired three new hygienists
Make no mistake: the gap between a trained FFS team and an untrained one isn’t 10%. It’s the difference between 45% case acceptance and 75% case acceptance. On a $50,000 unscheduled treatment month, that’s $15,000 in additional production.
Every month.
Compounding.
I tell every FFS client the same thing: stop sending your team to clinical CE. They have plenty.
Send them to communication CE. That’s the actual gap.
Pair every new hire with a mentor who’s already good at the FFS conversation, not just the team member who’s been there longest. Length of tenure doesn’t equal skill at value presentation. Sometimes it’s the opposite.
When was the last time you sat in on your treatment coordinator’s case presentations and gave her actual feedback?

How Do You Measure Performance In A Fee-For-Service Practice?
You measure performance in a fee-for-service practice by the metrics that drive margin, not volume. Case acceptance rate, production per patient, retention rate, and referral rate matter more than calls answered or rooms turned, because every FFS patient interaction has a higher revenue ceiling.
If your team doesn’t know what winning looks like, they won’t win. And in too many FFS practices, the KPIs being tracked are imported straight from the PPO playbook.
The Five KPIs That Matter Most In An FFS Practice
1. Case acceptance rate by dollar value. Not by number of patients. Track how much of your diagnosed treatment actually gets accepted and completed. Industry averages sit at 40-50% for general dentistry per Levin Group data. Your goal should be 70% or higher.
2. Production per patient visit. This tells you whether your hygienists and treatment coordinators are advocating for treatment or just running the schedule.
3. New patient retention rate at 12 months. FFS patients are harder to acquire and more valuable to keep. If your new patients aren’t coming back for their second hygiene appointment, your team is the leak.
4. Same-day treatment conversion. When hygiene identifies decay, what percentage gets treated the same day or scheduled within two weeks? This is a direct measure of your hygiene team’s value presentation.
5. Patient referral rate. FFS practices live and die by referrals because organic word-of-mouth is your lowest-cost acquisition channel. Track which team members are generating referrals, then figure out what they’re doing differently.
KPIs To De-Prioritize In An FFS Practice
- Room turnover time (this is a PPO metric)
- Calls answered per hour (volume, not quality)
- Number of new patients per month in isolation (if quality isn’t tracked alongside)
Schedule monthly performance check-ins, not as gotcha meetings, but as coaching sessions.
What’s working? What’s not? What support does the team member need to hit their KPI?

I’ve watched FFS practices add $200k+ in annual production just by switching the KPIs they track and the conversations those KPIs trigger. The work didn’t change. The focus did.
How Do You Keep A Fee-For-Service Dental Team From Quitting?
You keep a fee-for-service dental team by paying like your margin allows, building a culture that treats them as professionals not employees, and protecting them from the burnout patterns that destroy PPO offices. FFS practices have the financial room to invest in their people. The ones that don’t are wasting the entire model.
According to ADA HPI data published in early 2026, only 60% of dentists have an adequate number of dental hygienists on staff, and 91% of dentists actively recruiting hygienists said the process is very or extremely challenging. Replacing your A-player hygienist isn’t just inconvenient. It’s a six-figure problem when you factor in lost production, recruiting costs, training time, and patient relationship damage.
Granted, paying more isn’t a complete retention strategy. But it’s the floor. Here’s the rest.
Compensation That Reflects Your Margin
PPO practices fight over candidates at the bottom of the wage range because they can’t afford to pay more. You can. Use it.
Pay 10-15% above your local PPO average for FFS-trained staff, and you’ll attract candidates who otherwise wouldn’t apply.
Schedule Flexibility That Doesn’t Break The Practice
Four-day work weeks for clinical staff. Rotating Fridays off for front office. Predictable hours that let people have a life.
DentalPost’s 2026 Industry Salary Report found 56% of dentists are now working an average of four days per week, with burnout cited as a top driver. Your team feels the same pressure.
A Culture That Addresses Toxicity Instead Of Tolerating It
One toxic team member in a 6-person FFS practice damages a higher percentage of your patient relationships than the same person would in a 20-person PPO mill. The math is simple. Letting it slide costs you more here.
Real Investment In Their Development
Sponsor your treatment coordinator to attend AADOM. Pay for case presentation coaching. Cover communication CE that PPO offices won’t pay for.
Your team will notice, and so will your case acceptance rate.
Mental Health Support Backed By Behavior
Bring in a speaker once a quarter. Offer mental health days that don’t require explanation. Talk about burnout openly in team meetings.
Your team is managing anxious patients all day. They need somewhere to put that emotional weight down.
DentalPost’s 2025 Salary Report found that 37.5% of dental practice managers are actively pursuing a job change within the next few years, driven primarily by compensation, benefits, and work environment. If your FFS practice has the same turnover rate as a PPO mill down the road, what exactly are you offering your team that’s different?

How Do You Handle A Toxic Team Member In A Fee-For-Service Practice?
You handle a toxic team member in a fee-for-service practice by addressing the behavior immediately, specifically, and with documentation, because in a small high-margin practice, every patient relationship matters more. The cost of tolerance is higher here than in any PPO office.
Here’s the four-step approach that works.
Step 1: Call It What It Is
No “checking in,” no “touching base.” Open the conversation directly: “I need to talk to you about behavior I’ve observed that’s affecting the team and our patients. We need to address it now.”
Step 2: Bring Specific Evidence
Vague feedback won’t change behavior. Use exact examples: dates, situations, what was said or done. “Last Tuesday during the morning huddle, when Lisa raised the scheduling concern, you rolled your eyes and said ‘here we go again.’ That shuts down team collaboration, and it’s not acceptable here.”
Step 3: Set The Boundary And The Consequence
“Moving forward, I expect respectful communication in every team setting. If that doesn’t happen, we move to formal disciplinary action and possibly termination.” Document the conversation in writing, the same day.
Step 4: Offer One Path Back, Or The Exit
Some toxic team members can shift if they want to. Most don’t. Either way, the choice belongs to them, and the deadline belongs to you.
Don’t let “they’ve been here forever” become an excuse to keep losing your A-players.
The “they know the systems” defense is a hidden tax on your A-players. Every day your B-player toxic person stays, your A-players are watching and deciding whether to leave. They usually leave first.
Fire fast. FFS practices wait too long because the relationships feel more personal in a smaller office. That’s exactly the trap. The relationships with the rest of your team matter too.
What Exit Interview Questions Should A Fee-For-Service Practice Ask?
A fee-for-service practice should ask exit interview questions that surface culture gaps, leadership blind spots, and value-positioning weaknesses, not just generic “what could we have done better” prompts. Every departure is data your marketing budget can’t replace.
Use a neutral interviewer, ideally not the owner. Practice managers, HR contractors, or a trusted outside consultant get more honest answers than you will.
The Eight Questions That Actually Work
- What made you start looking for other opportunities? (Reveals the actual tipping point, which is rarely what you assume.)
- Was there a moment when you felt unsupported or unappreciated? (Surfaces leadership and culture gaps.)
- How would you describe the team culture here, in your own words? (Listen for “tense,” “competitive,” or “cliquey” as red flags.)
- Did this role align with what you were told during the interview? (Tells you whether your hiring conversations are honest.)
- What did you enjoy most about working here? (Double down on these strengths.)
- What was the most frustrating or unclear part of your job? (Could be a fixable process gap.)
- Was there anything we could have done that would’ve kept you? (Sometimes the answer is simple. Sometimes it’s revealing.)
- Would you recommend this practice to a friend looking for work? Why or why not? (The truest signal of how they actually felt.)
Time the interview on their last week, not their last hour. People are more honest when they have nothing left to lose. Document patterns across multiple exits and review quarterly.
One person’s complaint is noise. Three people saying the same thing is your culture problem.
Frequently Asked Questions About Hiring Dental Staff For A Fee-For-Service Practice
What do you still want to know about hiring A+ front office hiring staff?
What’s the average tenure of dental staff in a fee-for-service practice?
Tenure in well-run fee-for-service practices typically runs 3 to 5 years for clinical staff and 5+ years for front office and treatment coordinators, longer than the dental industry average. ADA HPI data shows staffing remains tied for the top challenge dentists face heading into 2026, and FFS practices that don’t invest in retention experience similar turnover to PPO offices.
How much should a fee-for-service practice pay a treatment coordinator in 2026?
Fee-for-service practices should pay treatment coordinators 10-15% above the local PPO average to attract candidates with case presentation experience. The DentalPost 2026 Industry Salary Report shows compensation continues to rise across all dental roles, with practice managers averaging $36.03 per hour in 2024 data and FFS-specific roles typically commanding a premium.
Do you need a dental hygienist with sales experience for an FFS practice?
You don’t need a hygienist with formal sales experience, but you need one comfortable with value-based treatment discussions. The skill matters more than the title. Most strong FFS hygienists were trained on the job, often by working alongside an experienced treatment coordinator and a doctor who models the conversation.
How long should the onboarding process be for a new FFS dental hire?
Onboarding for a fee-for-service dental hire should run 90 days, structured in 30-day phases focused on systems first, then communication training, then live patient interactions with feedback. PPO offices can get away with two-week onboarding because the job is mostly process execution. FFS offices can’t because the job is mostly conversation.
What’s the biggest hiring mistake fee-for-service practices make?
The biggest hiring mistake fee-for-service practices make is recruiting from the PPO talent pool without training for FFS skills.
A great PPO hygienist isn’t automatically a great FFS hygienist. The work is different and the conversation is different. Either train explicitly, or hire candidates with prior FFS experience.
Should I hire from a PPO practice or train from scratch?
Both paths work, but they require different commitments. Hiring from a PPO practice gives you faster clinical onboarding but requires deliberate retraining on value presentation, fee defense, and longer appointment formats. Training from scratch, especially new graduates from dental hygiene or assisting programs, takes longer but produces team members shaped entirely by your FFS culture.
How do I know if a candidate can handle the FFS conversation?
Test for it directly during the interview. Run a live scenario where the candidate role-plays a “do you take my insurance” call, or presents a $10,000 treatment plan to you cold. If they can’t hold poise during the test, they won’t hold it with patients. The resume can’t tell you. The role-play will.
Wrapping Up: Your Fee-For-Service Practice Doesn’t Have A Marketing Problem. It Has A People Problem.
Here’s the truth most dental marketing agencies won’t say out loud, including the ones you’ve probably hired before: you can’t market your way out of a bad team.
You can rank number one for every keyword that matters. Run perfect Google Ads. Optimize your GBP until it sings.
But if the right patient calls and talks to the wrong person at your front desk, or sits in the chair and gets a mediocre value presentation, none of it converts.
Every hire, every training session, every retention decision you make is a marketing decision in disguise.
Your team is the last mile between the patient your marketing brought in and the production that pays your overhead. That’s the load-bearing piece nobody talks about.
So start with one role. The one where the next bad hire would cost you the most. Fix that one first. Then handle your marketing.
This all may seem overwhelming and you don’t want to make a wrong move with such an important decision. So why not get help from professionals? Like Practiwrite.
Start by scheduling your 100% free Dental Practice Roadmap. Your Dental Practice Roadmap is a GBP and website audit that shows you exactly where you stand, what keywords you’re ranking for now, what you should be ranking for, and a step-by-step plan to close those gaps.
Because here’s what I see over and over: practices spend years fixing their team only to discover their marketing was the real bottleneck. Or they fix marketing only to watch the new patients leak out through a poorly trained front desk.
Your team and your marketing have to work together. The Roadmap shows you the marketing half in plain numbers, no fluff.
No vague recommendations. No generic dental marketing advice. Just a clear picture of what’s broken and what to do about it.
Book your Dental Practice Roadmap and get yours now.
10+ year content strategist, writer, author, and SEO consultant. I work exclusively with dental practices that want to grow and dominate their local areas.