Most dentists planning how to drop a PPO plan obsess over the same thing.
They write a script.
They rehearse it.
They train the team.
They lose sleep over what their hygienist will say when a longtime patient asks why their insurance isn’t accepted anymore.
Then they drop the plan, lose patients anyway, and can’t figure out what went wrong.
Here’s the truth nobody in dental marketing wants to say out loud. The patients who leave after a PPO drop aren’t reacting to what your team said in the chair.
They’re reacting to what your website, GBP, voicemail, and social profiles were already telling them when they went home and fact-checked the conversation.
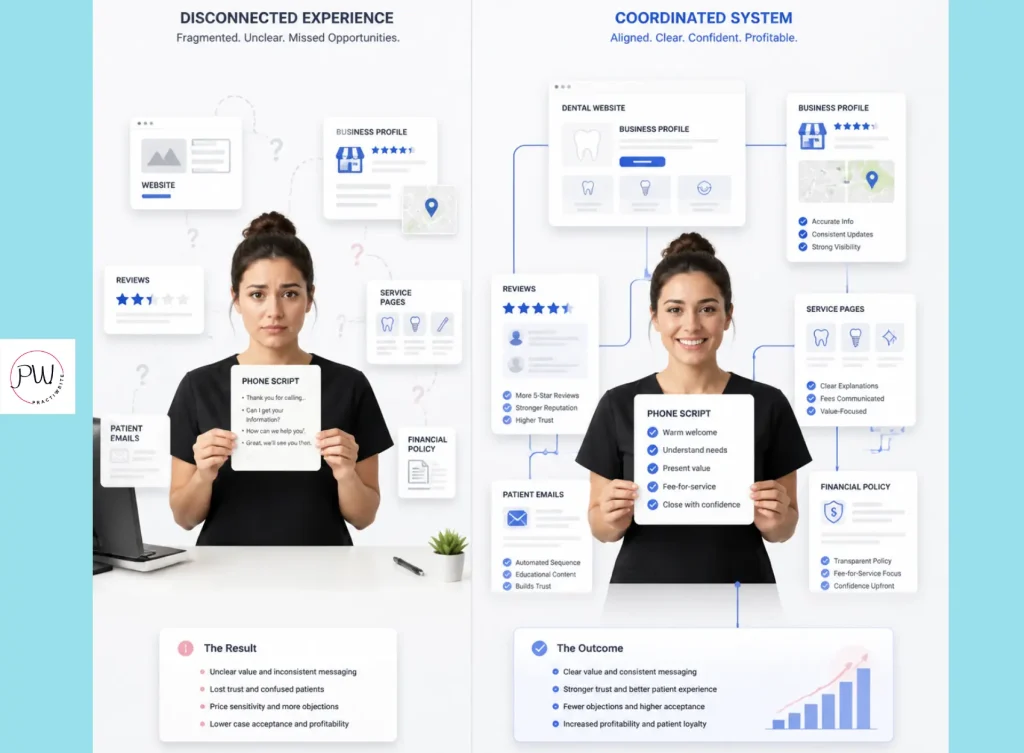
The operatory script is one of seven patient touchpoints.
The other six are running the show.
If you’re trying to figure out how to drop a PPO plan without losing your best patients, the answer isn’t a better script. It’s alignment across every place a patient can verify what your team just told them.
Patient retention isn’t even the right goal. Patient sort is. The right patients leave during a PPO drop.
The wrong dentists try to keep them all.
Why Do Most Dentists Get the PPO Drop Conversation Wrong?
Dropping a PPO plan is the act of terminating your in-network contract with a specific dental insurance carrier. The communication challenge isn’t the act itself. It’s everything you say, and everything you don’t say, around the act.
Here’s what most dental marketing agencies tell dentists to do:
- Write a script
- Train the team
- Send a letter
- Done
It’s tidy advice. It’s also missing about 85% of what actually drives patient retention.
Patients don’t take your team’s word for it.
They go home. They pull up your website at 9pm. They check your Google Business Profile. They look at your social bios.
And if anything they find contradicts what your team just told them in the operatory, your team’s words become suspicious.
When the conversation in the chair and the digital storefront tell two different stories, patients default to the digital. They can re-read your website at midnight. They can’t re-listen to your hygienist.
So whatever your website says is what becomes true.
I’ve audited dozens of practices in the middle of going fee-for-service, and the contradictions almost always live in the same three places:
- The homepage hero section
- The GBP services section
- The insurance page that’s still sitting on the website from three years ago
Most dentists don’t even realize the old insurance page is still live.
That’s where retention bleeds out. Not in the operatory. On the parts of your digital presence you forgot you owned.
When was the last time you read your own website the way a confused patient would?
Is Patient Retention the Wrong Goal When Dropping a PPO Plan?
Patient retention measures how many patients stay. Patient sort measures who stays and who leaves. The right fee-for-service transition optimizes for the second, not the first.
Here’s the math nobody runs. If you keep 95% of your patient base but the 5% who left were your highest-value cases, you lost. If you keep 75% but the 25% who left were the fee-haggling, treatment-declining, no-show patients, you won.
Retention as a single number is a vanity metric. The question that matters is which patients stayed.
The patients who leave during a PPO drop usually share a few traits:
- They chose you because of the insurance directory, not the dentistry
- They fight every fee
- They decline anything not fully covered
- They no-show
- They’re the patients your front desk dreads.
The patients who stay are different.
They value the dentistry over the discount. They accept comprehensive treatment plans. They refer friends. They write reviews. They’re the patients your new economic model needs.
This is why the sort matters. The dentists who fight to keep every patient are also the ones who can’t escape the contracts that are squeezing them. The dentists who accept the sort and run it cleanly end up with a smaller patient base that funds more dentistry, not less.
Every fee-for-service practice I’ve worked with had the same blind spot before transition. They were terrified of losing the wrong patients. Six months later, they were embarrassed they ever wanted to keep them.
Which would you rather keep: 100% of a patient base that’s bleeding you, or 75% of one that’s funding the practice you actually want to run?
What Are the Seven Touchpoints Patients Use To Fact-Check Your Script?
A patient touchpoint is any place a current or prospective patient interacts with your practice. The seven that matter during a PPO drop are the ones a patient can verify on their own, without your team in the room.
Listed in order of how often patients check them after the in-office conversation:
- Website homepage
- Google Business Profile services section and description
- Website insurance page, if it still exists
- Voicemail and after-hours message
- Social profile bios on Facebook and Instagram
- Intake forms and new patient paperwork
- Review responses on Google and Yelp
What are patients actually looking for when they check? Confirmation or contradiction.
They’re not reading your website for marketing copy. They’re reading it for proof of what they just heard.
Every word becomes evidence. Every phrase gets weighed against what your team said.

The touchpoint most dentists miss is the seventh one. Review responses.
When a frustrated patient leaves a review saying “they don’t take my insurance anymore,” your response becomes public marketing copy. It’s now permanently indexed on Google. Every future prospect who reads that review will also read your response.
If you sound defensive, every prospect learns to be suspicious. If you sound apologetic, every prospect learns the change was a mistake. If you sound confident and clear, every prospect learns the drop was deliberate and the practice stands by it.
If a patient drove home from their last cleaning and pulled up your website tonight, would they find the same story your team just told them?
What Should the In-Office Script Sound Like (And Why Is It Smaller Than You Think)?
The operatory script is the conversation your team has with patients in person about the insurance change. It still matters. But it’s the smallest of the seven touchpoints, not the largest.
A good script hits five beats in order:
- Empathy
- Plain-language explanation
- Patient benefit
- Next steps
- Objection handling
Empathy first:
“I wanted to talk with you personally because I know your care here matters to you. There’s a change in how we work with your insurance plan, and I want to walk you through what it means for you.”
The change, plain language:
“As of [date], we’re no longer a contracted provider with [Plan Name]. Your plan still works here. We just won’t be bound by what the plan limits us to.”
Patient benefit:
“This means we can recommend the care we actually believe is best for you, not what an insurance company decides should be covered. You’ll still use your benefits. We’ll still file your claims.”
Next steps:
“At your next visit, the care doesn’t change. You pay us at the time of service. Your insurance reimburses you directly. We help with the paperwork.”
Objection handling, short and direct:
“Will it cost more?” Slightly different in some cases, and we walk you through the numbers before treatment. “Can I still see you?” Yes. “Why are you doing this?” So we can recommend the care you actually need without the plan deciding for us.
Here’s the cheat sheet your front desk needs at their station:
- Don’t say “We don’t take your insurance anymore.” Do say “We’ve stepped outside the network so we can deliver the care we believe in.”
- Don’t say “Sorry about that.” Do say “I understand this is a change. Here’s how it works now.”
- Don’t say “It’s a billing thing.” Do say “We made this decision so we can put care first.”
The team’s job isn’t to memorize a paragraph. It’s to internalize three beats: acknowledge the change, frame the benefit, reassure on next steps. One message, one voice, every conversation.
But the part nobody else will tell you is that even a perfect operatory script can’t repair contradiction at the digital touchpoints. The script is downstream of alignment, not the cause of it.
If your script is perfect but your website still lists Delta in the footer, which one is the patient going to believe at 9pm tonight?
What Should Your Website and GBP Say When You Drop a PPO Plan?
Website and GBP alignment means every page, listing, and public-facing description tells the same story your team tells in the chair. This is where most PPO drops succeed or fail.
The homepage hero section is the first thing patients see when they go to fact-check.
What has to come off:
- Any mention of accepted PPO insurance
- “We work with most plans“
- “Affordable care for everyone”
- And any language that signals price-first positioning
What has to go on: language that signals quality, judgment, and experience.
Talk about outcomes. Talk about case complexity. Talk about the kind of dentistry you do, not the insurance you accept.
The insurance page is the single biggest contradiction trap. Most fee-for-service practices should either delete the page or replace it with an Out-of-Network Care page that explains your billing process clearly.
The goal isn’t nostalgia about who you used to contract with. The goal is clarity about how the relationship works now. List the carriers you still file claims with as a courtesy.
Explain reimbursement. Explain payment at the time of service. Explain that you’ll help with paperwork. Done.
Complete Overhaul of your GBP Services and Description
The GBP services section needs a full rewrite. Remove any PPO-coded language from your service descriptions. Update the Q&A. Refresh photos if any showed insurance-related signage.
Add language about case quality, advanced procedures, and the kind of patient your practice is built to serve.
The GBP description is the single most-read piece of copy a local patient will encounter before deciding to call your office. It deserves more attention than most dentists give it.
Lead with your positioning, not your services menu. Lead with what makes your practice different, not what makes it the same as every other practice in town.
Based on My Own Research of 2,000 Dental Practice GBPs
My original research across thousands of dental practice Google Business Profiles found that the practices ranking highest for high-intent fee-for-service searches share three specific traits in their GBP description. None of them mention insurance. Two of them mention the kind of patient the practice is built for.
All three lead with a verb that signals action, not a noun that signals a list. That’s the pattern.

If a patient who’d never met you read your website cold today, would they think you’re a fee-for-service practice or a PPO practice?
How To Drop a PPO Plan: What Does a 60-Day Touchpoint Alignment Timeline Look Like?
A touchpoint alignment timeline is the sequence of changes you make across all seven patient touchpoints before your PPO drop date. The goal is full alignment by day one of the drop, not 30 days after.
Here’s how to drop a PPO plan in 60 days without leaving any touchpoint unaligned.
Days 60 to 45: Digital First
This is the longest stretch because digital takes the most time and gets the most fact-checking. Rewrite the website homepage. Replace or delete the insurance page.
Update the GBP description and services section. Refresh the voicemail. Update Facebook and Instagram bios.
Take down anything that contradicts the new positioning. If you start anywhere else first, the rest of the timeline runs on borrowed time.
Days 45 to 30: Internal Alignment
All-hands team meeting. Walk every team member through the change, the why, and the script.
Role-play the top three patient objections. Update intake forms to reflect the new billing process. Brief any associate doctors.
By the end of this phase, every person who picks up the phone should know exactly what to say.
Days 30 to 15: Patient Communication Launch
Send the patient letter to everyone in the affected plan. Personal phone calls to your top-value patients. In-office conversations begin for anyone who walks in during this window.
Patients now have three different ways the message is hitting them. The website backs it up. The voicemail backs it up. The team backs it up.
Days 15 to Drop Date
Personal outreach to high-value patients with appointments scheduled after the drop. Final website and GBP audit. Walk through every page like a confused patient would.
Check the footer. Check the contact page. Check the FAQ.
Make sure nothing has slipped back into PPO-coded language.
Day One of The Drop
A social media post announcing the change is live. Final email reminder. Any last-minute updates to the homepage.
Every touchpoint now tells the same story.
What’s the point of a 60-day plan if days one through 45 are spent perfecting the script and only day 46 onward touches the website?
What Does Patient Sort (Not Patient Retention) Actually Look Like?
Patient sort is the natural self-selection that happens when a practice’s positioning becomes clear and consistent. After a PPO drop, the patients who leave are signaling that they were never the right fit.
Three practices that ran the sort cleanly:
Practice 1, suburban Colorado:
A five-operatory general practice dropping two low-reimbursement PPOs. They gave 90 days’ notice. But they also rewrote their homepage and updated their GBP in that same 90 days.
By the time patient letters went out, every touchpoint was already telling the new story.
The team’s script wasn’t inventing anything. It was confirming what patients had already seen. They retained 83% of affected patients, and case acceptance went up 7%.
Practice 2, rural Tennessee:
A solo dentist dropping one major PPO. The team was nervous and obsessed over the script. They also updated their GBP, refreshed services descriptions, and replaced the insurance page with an out-of-network billing explanation.
They lost 12% of affected patients. The ones who stayed told the front desk how “professional” the change felt. What they were responding to was alignment.
Practice 3, downtown Chicago:
A boutique fee-for-service practice dropping its last in-network plan. They recorded a 90-second video from the dentist, posted it on the homepage, and sent it by email. The video had a 72% open rate.
They retained 88% of affected patients. The video didn’t carry the retention. The aligned digital presence behind it did.
The pattern in all three: the operatory script wasn’t doing the heavy lifting. It was confirming a story the digital touchpoints had already told.
Now the numbers behind the sort itself. In aligned transitions, the 12% to 17% of patients who leave are almost entirely concentrated in the lowest-value cohort. The retained 80%-plus tend to be patients who were already aligned with quality-first care. Average revenue per patient often climbs 30% to 50% in the year after transition, because the remaining mix is heavier on case acceptance and lighter on no-shows.
This isn’t loss. It’s sort.
If 18% of your patients leaving means your average production per patient jumps 40%, did you lose patients or did you finally start running the practice you wanted?
What Common Mistakes Break the Alignment Between Touchpoints?
Alignment mistakes are the small inconsistencies between touchpoints that undo a well-executed PPO drop. Five show up most often.
Mistake 1: Waiting too long to start digital changes
Most dentists give themselves 60 days for the team and zero days for the website. The digital touchpoints need the full 60. If you start the website rewrite when the patient letters go out, you’ve already lost the window.
Mistake 2: Hiding behind jargon in the website rewrite
“Network terminations” and “out-of-network reimbursement protocols” don’t communicate anything to a patient. Plain language is the goal everywhere, not just in the operatory.
Mistake 3: Inconsistent messaging across touchpoints
The website says one thing. The GBP description says another. The voicemail says a third. The Facebook bio still mentions PPO acceptance from 2022. Patients notice every mismatch.
Mistake 4: Sounding defensive in review responses
The first negative review after a PPO drop is a stress test. If you respond with explanations and apologies, every future prospect reads a practice that wasn’t sure of the decision. If you respond with clarity and confidence, every future prospect reads a practice that stands by it.
Mistake 5: Forgetting to brief the team on the digital changes
Your hygienist should know what the website says. Your front desk should know what the GBP description says. If a patient quotes the website to a team member and the team member doesn’t recognize it, the contradiction lands at the worst possible moment.
Are you running a fee-for-service practice, or just a PPO practice with a new script?
Frequently Asked Questions About Dropping a PPO Plan
What do you still want to know about dropping a PPO plan? Let’s get some answers:
How long before the drop date should you notify patients about dropping a PPO plan?
60 to 90 days. This gives patients time to process, ask questions, and adjust. It also gives you time to align every other patient touchpoint before they start fact-checking your team’s script.
Should you mention the dropped insurance on your website?
Yes, but not the way most dentists do it. Don’t list the dropped plan by name. Replace your insurance page with an Out-of-Network Care page that explains your billing process. The goal is clarity about how billing works now, not nostalgia about who you used to contract with.
What percentage of patients typically leave after a dental practice drops a PPO plan?
Between 10% and 17% in well-aligned transitions, concentrated in the lowest-value patient cohort. Practices with misaligned digital touchpoints often lose more, sometimes 30% to 40%, because patients lose trust when the website contradicts the team.
What’s the biggest mistake dentists make when dropping a PPO plan?
Treating the operatory script as the only deliverable. The script is one of seven patient touchpoints. The website, GBP, voicemail, and review responses are the others. If those contradict the script, patient retention drops sharply.
How should your Google Business Profile change when you drop a PPO plan?
Update the business description to lead with quality-first positioning, not insurance acceptance. Rewrite the services section to remove PPO-coded language. Refresh the Q&A. Update photos if any showed insurance-related signage.
Can you keep some PPO contracts and drop others?
Yes. This is called a hybrid model, and it’s a common transition path for practices that don’t want to go fully fee-for-service immediately. Patient communication still needs to be precise about which plans you dropped and which you kept, both in operatory conversations and on the website.
What’s the right script for telling existing patients you’re dropping their insurance?
Open with empathy. Explain the change clearly without jargon. Frame the benefit to the patient. Outline next steps. Handle common objections directly. Keep it short, conversational, and confident. But remember: the operatory script is one of seven patient touchpoints, and it’s the smallest. Your website, GBP, voicemail, and review responses all have to confirm the same story.
Wrapping Up: How To Drop a PPO Plan and Keep the Right Patients
The PPO drop conversation isn’t a script problem. It’s an alignment problem.
The patients who leave after a drop aren’t reacting to what your team said in the chair. They’re reacting to what your website didn’t back up when they went to verify.
Spend 60 days perfecting the script and ignoring the other six touchpoints, and you’ll lose more patients than you needed to. You’ll also lose the wrong ones.
Align all seven, and the patients who leave are exactly the ones your new model is built to release. The ones who stay are the ones who fit.
That’s the difference between a PPO drop that breaks a practice and one that finally lets the practice run the way you’ve always wanted.
Now decide whether your current patient touchpoints are aligned with the practice you’re trying to build, or with the one you’re trying to leave behind. If you don’t know the answer, that’s the answer.
Want someone to help you with your FFS Transition? Let Practiwrite help by scheduling your 100% free Dental Practice Roadmap.
Your Dental Practice Roadmap is a GBP and website audit that shows you exactly where you stand, what keywords you’re ranking for now, what you should be ranking for, and a step-by-step plan to close those gaps.
No vague recommendations. No fluff. Just a clear picture of what’s broken and what to do about it.
Book your Dental Practice Roadmap and get yours now!
10+ year content strategist, writer, author, and SEO consultant. I work exclusively with dental practices that want to grow and dominate their local areas.