Here’s the real math. There’s no flat percentage that answers how much a fee-for-service practice should spend on marketing.
The right number comes from two things: what a new patient is worth to you, and what it costs to acquire one.
Set your fee-for-service dental marketing budget that way and it usually lands between 5% and 8% of collections in steady state, and higher during a growth push or a PPO transition.
But the percentage is the output, never the input.
Copy the “3 to 5% of revenue” rule every agency repeats and you’ve already lost, because that rule was built for practices that run on volume. Yours doesn’t.
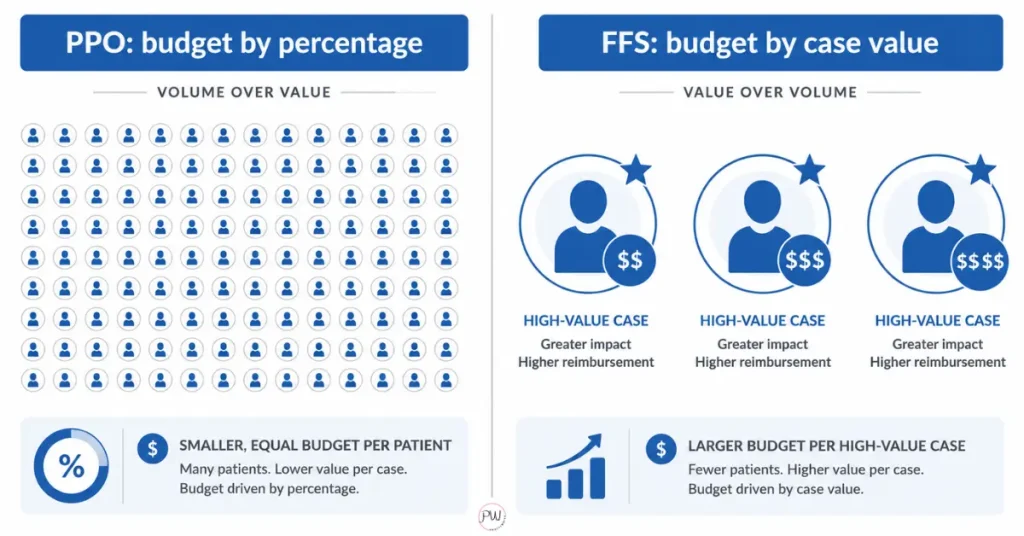
PPO practices fill chairs with interchangeable, low-margin visits, so a percentage rule fits them fine. Every patient is worth about the same, so you budget like a factory.
Fee-for-service is a different sport. One implant, one full-arch, one cosmetic case can be worth twenty to forty routine cleanings.
When your patients aren’t interchangeable, budgeting like they are either leaves money on the table or pours it down the drain. Two practices can bank the exact same collections and still need wildly different budgets, and the percentage rule can’t see why.
So the honest answer to “how much should I spend” is a better question: what’s a new high-value patient worth, and what does it cost to land one? Answer those two and the budget builds itself.
The rest of this post is the real math on how.
Table of Contents
How Much Should A Fee-For-Service Practice Spend On Marketing?
A fee-for-service practice should spend enough to consistently acquire its target number of high-value cases at a profitable cost per case. For most practices that works out to a range, not a fixed figure: commonly 5% to 8% of collections in steady state, and 10% or more during a growth phase or a PPO transition. The number is a result, not a starting point.
Why a range instead of one tidy number? Because two FFS practices with identical collections can have wildly different right answers. It depends on case mix, how competitive your market is, and how strong your visibility already is.
A practice that already ranks well and owns its local search needs less. A practice starting from a thin Google Business Profile and a weak website needs more, because it’s buying its way out of a hole first.
Why The “Percentage Of Revenue” Rule Is A PPO Answer To An FFS Question
The percentage-of-revenue rule says spend a fixed share of collections, usually 3% to 5%, on marketing. It’s the default advice in dentistry, and for a PPO practice it holds up. For a fee-for-service practice, it’s the wrong tool for the job.
Here’s the flaw. The percentage model assumes every patient is worth about the same, so spend scales neatly with revenue.
That assumption works when you run on volume and someone else sets your fees. It collapses the moment your patients stop being interchangeable.
A PPO practice spending 4% to fill the schedule with capped-fee cleanings is playing a volume game. A fee-for-service practice is playing a value game, where landing three implant cases this quarter can matter more than booking thirty hygiene visits.
Budget by percentage and you’ll quietly underspend on the high-value cases that actually drive an FFS practice, because the math sizing your budget is blind to what each patient is worth. We’ve watched practices anchor to 4%, then wonder why the cosmetic chair sits empty.
The budget wasn’t too small for a PPO practice. It was the wrong shape for an FFS one.
What’s The Real Math? Case Value Versus Patient Acquisition Cost
The real math is simple. Take what a new patient is worth to your practice (case value, or better, lifetime value) and divide your marketing spend by the number of new patients it produces (patient acquisition cost). If case value dwarfs acquisition cost, you spend more, not less.
Run it. Say a single implant case is worth $4,500 in production, and it costs you $600 in marketing to acquire that patient. That’s a 7.5 to 1 return on one case, before you count the hygiene, the referrals, and the second arch two years later.
Now picture that same $600 spent to land a cleaning capped at $90 after the write-off. Disaster. Different patient, different math, different budget.
This is exactly why “spend less” is such bad advice for FFS practices. When acquisition cost is low relative to case value, every additional dollar you can profitably deploy is a dollar you should deploy. The constraint isn’t your budget. It’s how many profitable cases your market can actually supply.
How Do You Set A Fee-For-Service Dental Marketing Budget?
You set a fee-for-service dental marketing budget by working backward from a case-acquisition goal, then allocating across the channels that produce those cases, split between building visibility and maintaining it. Don’t start with a number. Start with a target.
Step One: Pick Your Case Target
How many high-value cases do you want next quarter, and what’s each worth? That’s your revenue goal.
Step Two: Estimate Acquisition Cost Per Case
Pull it from your own numbers, or use a realistic benchmark if you don’t have data yet.
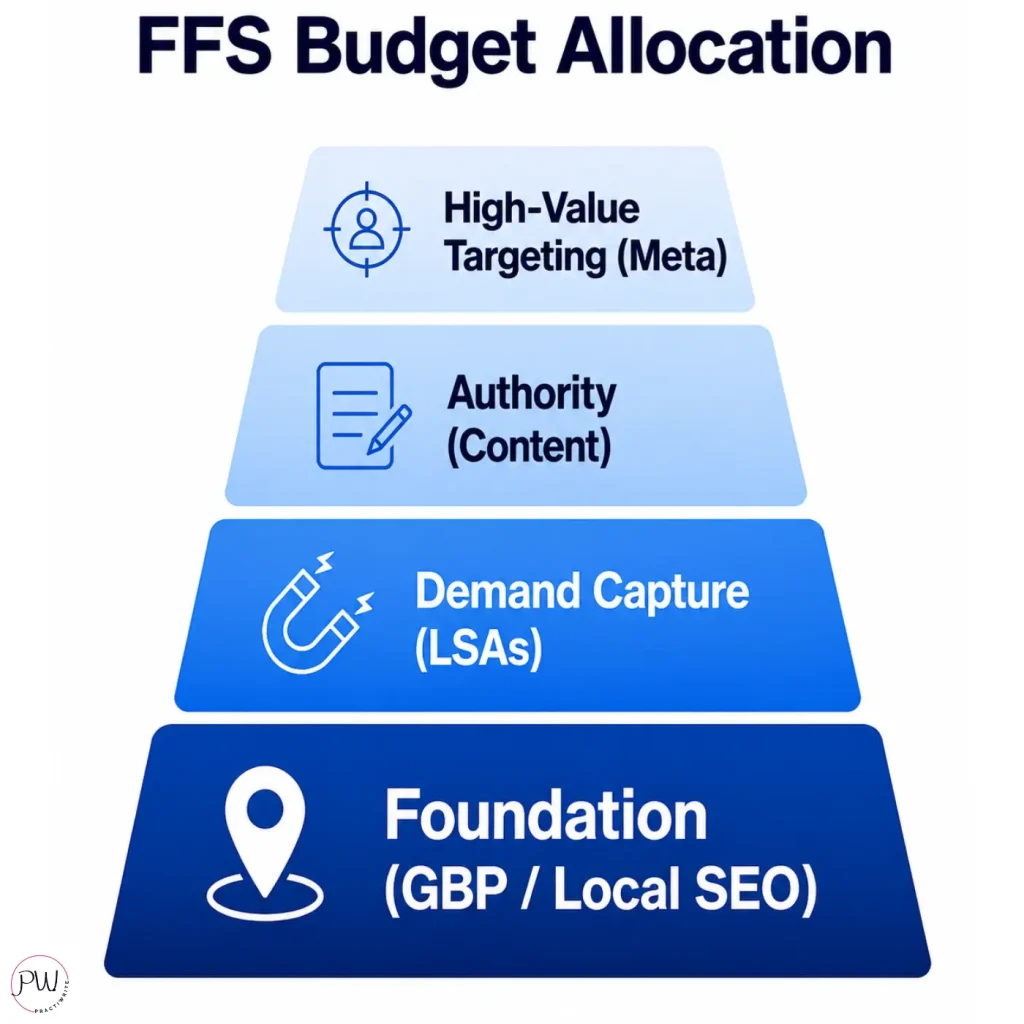
Step Three: Allocate In Layers, Not One Line Item
- Foundation (Google Business Profile and local SEO): non-negotiable, and where acquisition starts. Most of your early budget belongs here.
- Demand capture: pay-per-lead, so you pay when a patient actually calls. Predictable and measurable.
- Authority (strategic content): the asset that compounds, ranks in Google and in LLMs, and pre-sells the patient before the call.
- High-value targeting (Meta ads for cosmetic and implant cases): the layer that goes after the specific high-margin cases worth the most.
The split shifts over time. Early on you spend heavier to build, catching your visibility up. Once the foundation ranks, more of the budget moves to capture and maintenance.
A practice that spends like it’s building forever wastes money. One that stops building too early never gets off the ground.
Before you hand any of this to an agency, read what to ask before hiring a dental marketing agency.
What’s The Minimum A Fee-For-Service Practice Should Invest?
The minimum is the point below which you can’t sustain enough visibility and demand capture to acquire cases faster than you lose patients to normal attrition. Below that floor, you’re not running an FFS strategy. You’re running a PPO strategy with fewer patients and no network feeding you.
I’ll be straight: there’s no universal dollar floor, but in most competitive US markets a serious FFS practice underfunds itself below roughly $3,000 to $5,000 a month all-in, once you account for foundation, capture, and the tools to track it. Granted, that’s real money, and writing that check stings when you’re used to a network handing you patients.
Here’s the trade-off, in plain terms. Spend below the floor and you’ll get volume-practice results: thin visibility, inconsistent leads, and a marketing line you’ll eventually cut because “it didn’t work.” It didn’t work because it was never funded to work.
Underfunded marketing doesn’t fail quietly. It fails expensively, by convincing you the strategy was wrong when the budget was just too small.
What About Practices Transitioning From PPO To FFS?
Practices transitioning from PPO to FFS should plan to spend more on marketing during the transition, not less, because you’re replacing the patient flow a network used to provide with patient flow you generate yourself. Cutting marketing mid-transition is the single fastest way to empty your chairs and then blame fee-for-service for it.
Think about what’s actually happening. You’re walking away from a referral engine, the network directory, that for all its flaws sent you bodies. The day you drop a plan, that flow stops.
Your marketing has to be strong enough to replace it before the gap shows up in your schedule. That means spending ahead of the cut, not after it.
This is exactly where practices that “tried fee-for-service and it didn’t work” went wrong. They dropped the plans, kept the same thin marketing budget, watched new patients dip, and panicked.
Going fee-for-service didn’t empty their chairs. Marketing built for the wrong practice did.
For the full mechanics, see why most PPO-to-FFS transitions fail.
How Do You Know If Your Marketing Budget Is Actually Working?
Your marketing budget is working if you can trace spend to production: new high-value cases booked, revenue per channel, and cost per acquired patient trending the right way. If you can’t tie dollars to cases, you don’t have a budget. You have a guess wearing a budget’s clothes.
The trap is vanity metrics. Impressions, likes, “engagement,” follower counts. None of them pay your overhead.
A campaign can rack up reach and produce zero cases, while a quiet Google Business Profile optimization produces ten. Plenty of agencies report on vanity metrics precisely because those numbers always go up and never get them fired.
That’s the gap I wrote about in why most dental marketing agencies fail fee-for-service practices. Production attribution is harder, less flattering, and the only thing that matters.
So measure what moves money. Which channels produce calls. Which calls become appointments. Which appointments become high-value cases. What each of those cost. Watch those instead of the pretty numbers and your budget stops being a leap of faith and starts being a lever you pull with confidence.
Wrapping Up: FFS Practice Marketing Spend Is About Case Value
Here’s the whole thing in one line: the dentist asking “how little can I spend on marketing” already lost, and the one asking “what’s my return per dollar” already won.
Budget by percentage and you’ll fund a volume practice you don’t run. Budget by case value and acquisition cost and you’ll fund the one you actually have, the one that runs on quality. Stop shopping for the cheapest marketing and start buying the most profitable.
But you can’t budget by return if you don’t know where you stand right now. You can’t calculate acquisition cost if you don’t know what you’re ranking for, what you should be ranking for, or where patients are slipping through the cracks. That’s exactly what the Dental Practice Roadmap shows you.
Schedule your 100% free Dental Practice Roadmap.
Your Dental Practice Roadmap is a GBP and website audit that shows you exactly where you stand, what keywords you’re ranking for now, what you should be ranking for, and a step-by-step plan to close those gaps.
No vague recommendations. No fluff. Just a clear picture of what’s broken and what to do about it.
Book your Dental Practice Roadmap and get yours today now.

10+ year content strategist, writer, author, and SEO consultant. I work exclusively with fee-for-service dental practices that want to build value, not volume.